

RA is a systemic autoimmune disease affecting approximately 0.5–1% of the population. The disease involves damage to joint cartilage and bone; it is progressive in nature and characterised by inflammation and destruction, which can lead to long-term joint stiffness and instability.
In recent decades, significant progress has been made in the availability of therapies and validated disease-monitoring scales, as well as in terms of clinical guidelines and the treat-to-target strategy. Joint damage is irreversible, so early and effective treatment is of paramount importance. Clinical guidelines recommend remission, or at least low disease activity.
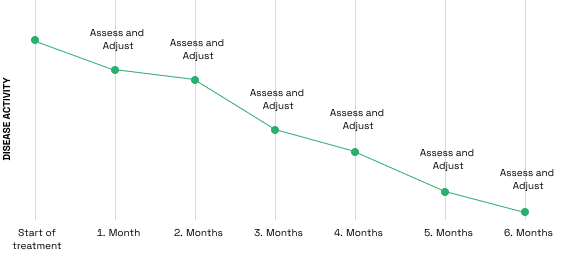
The ‘treat-to-target’ strategy can prevent RA-related disability and can lead to improved outcomes
Recommended: frequent assessment of disease activity and adaptation of treatment if necessary
Several tools are available for monitoring disease activity and progression (e.g. DAS28, SDAI, CDAI); these are widely used and contain both objective and subjective elements. Structural damage, which is the main factor determining the course of the disease, can be assessed using imaging techniques.
Several risk factors for radiographic progression are known, including high disease activity, which can be monitored using non-specific inflammatory markers such as erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), rheumatoid factor (RF) and anti-citrullinated protein antibody (ACPA; most commonly anti-CCP) seropositivity. However, these parameters may fall within the normal range whilst joint destruction progresses, raising the need for additional biomarkers. In recent decades, significant progress has been made in the availability of therapies and validated disease-monitoring scales, as well as in terms of clinical guidelines and the treat-to-target strategy. Joint damage is irreversible, so early and effective treatment is of paramount importance. Clinical guidelines have set remission, or at least the achievement of low disease activity, as the target.
Features:
For diagnosis or to monitor therapeutic response, results must always be interpreted in conjunction with the patient’s medical history, clinical examinations and other findings!
In Hungary, MMP-3 level testing is available nationwide on a self-funded basis through the SYNLAB blood collection network and at all private healthcare providers contracted with SYNLAB.
In other European countries, MMP-3 will be available soon.